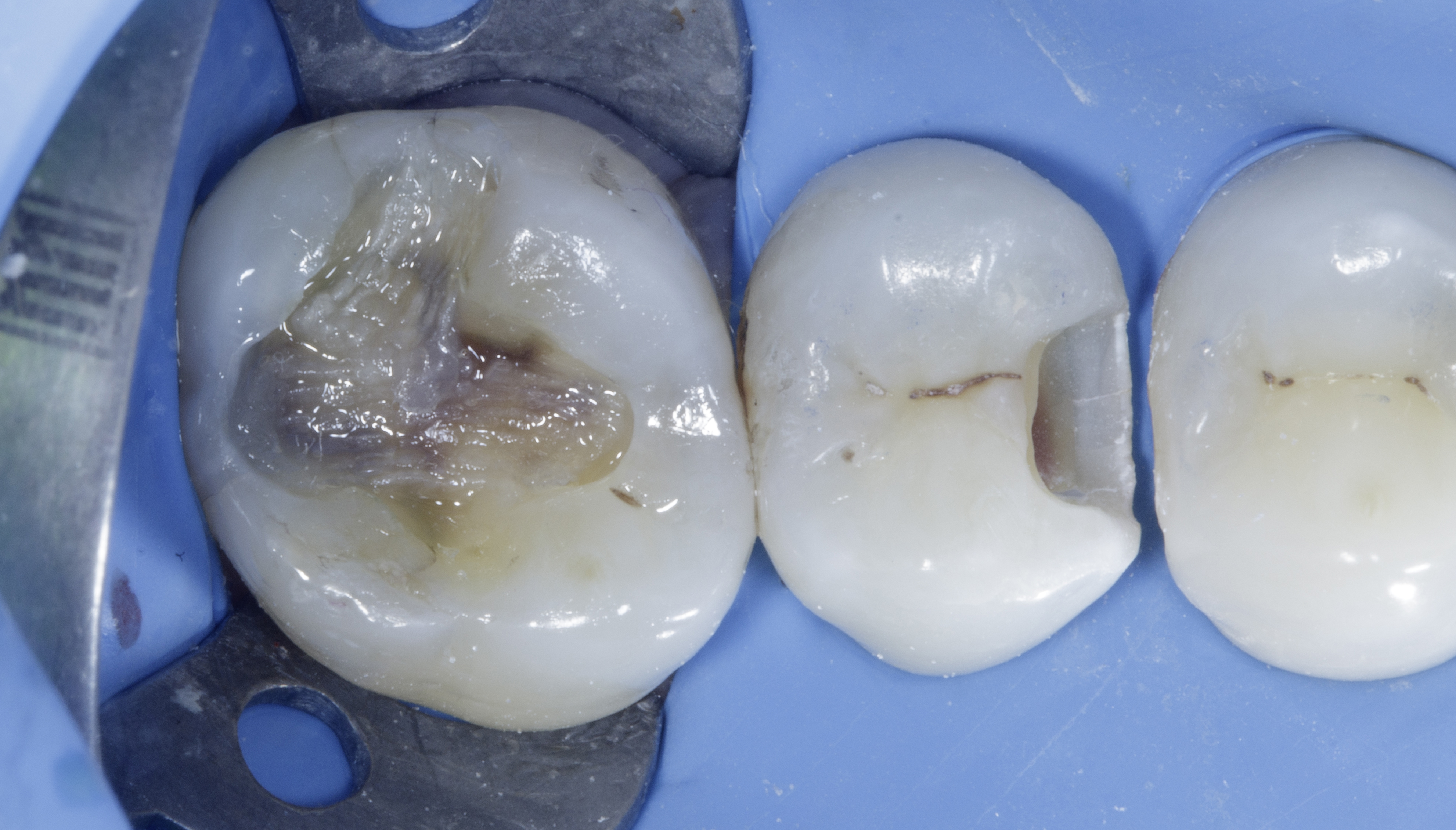
We began by using a small round bur to initiate drilling on tooth #15 at the suspected entry point along the mesial groove and discovered a typical Class II carious lesion (Figure 4). We then decided to place a rubber dam before proceeding with the rest of the treatment.
Rubber Dam Isolation achieved using a wingless clamp with heavy rubber dam to achieve optimal bonding and increase the longevity of the restoration. Proper isolation is crucial for a successful adhesive process.
Silver/ Caries Removal: Silver restoration removed carefully using high speed round bur. Utilize caries dye for the thorough removal of carious tissue in teeth #15/#16 (Figure 5), infected caries is removed using slow speed round carbide bur with use of caries dye. It is essential to establish a peripheral seal zone free from infected and affected dentine to ensure the best bonding strength.
|
|
|
|
Figure 4. After initial drilling as suspected classical Class 2 defect.
| Figure 5. After removal of silver amalgam restoration / decay from tooth #16. Where as #15 shows infected dentine highlighted by caries dye.
| Figure 6. After Caries removal, achieving peripheral zone and air abrasion, ready to restore.
|
Enamel / Proximal Box Preparation: Remove all unsupported enamel using a Super Fine Diamond Bur (yellow band). Contact broken in order to place the matrix band perfectly.
Finish the proximal walls with Shofu Super-Snap disks: start with the violet disk, followed by green and pink disks. This approach ensures optimal bonding to the enamel and helps prevent potential microleakage. Air particle abrasion using 25-micron aluminum oxide powder for more than 5 secs. This process cleans the cavity preparation and enhances bonding strength. Figure 6
We began with restoring first tooth #16 , After applying the bonding agent, we used a thin layer of Shofu Injectable Xsl—a high-strength, self-levelling, 2nd generation injectable material—to seal the dentine. This initial layer, approximately 0.5 mm thick, is crucial for protecting the hybrid layer from shrinkage stress. The self-levelling properties of this material allow it to effectively adapt to uneven surfaces, ensuring a smooth application without air bubbles and minimizing post-operative sensitivity…..NO CURE. Then we placed Ribbond Fibers (dipped in the unfilled resin) in 2 directions as per the cavity design and then cured all together. Figure 7
|
|
Figure 7. Ribbond Fiber placement in 02directions as per the defect along with thin layer of Shofu Injectable Xsl A2O shade.
|
Ribbond fibers are ideal in Class I cavities due to High C factor, this will even reinforce the composite restoration and improve its fracture resistance — especially in teeth that are structurally compromised or wider defect like in this case.
- Crack resistance: The polyethylene fiber mesh resists crack propagation within the composite, increasing longevity of the restoration
- Stress distribution: Ribbond helps distribute occlusal stresses more evenly across the restoration and tooth structure.
After the protecting hybrid layer, we began incremental, cusp-by-cusp morphological layering technique. using Shofu Bioactive composite Shade A2. Figure 7. Once these restorations were completed, we proceeded to the critical step of addressing the Class II defect on tooth #15.
Selecting the appropriate sectional matrix system is crucial in class 2 defect cases so we chose Garrison Quad system. It is not true that the Quad matrix system can be used only for adjacent class 2 defects. It works very well in single class 2 as well more efficiently.
It is essential to ensure that the marginal ridge is correctly dimensioned and aligns with the occlusal anatomy. This alignment is vital for creating well-defined adjacent triangular fossae and a properly shaped occlusal embrasure. Therefore, the height of the marginal ridge largely depends on the choice of band height. Here we chose Firm band FXH 175
The firmness of the band material facilitates easy placement and secure fitting, the bands maintain their shape and do not distort during layering the composite ensuring accurate and reliable restoration outcomes. The band is secured with a Quad blue wedge, selected based on fitting firmness - a larger wedge is chosen if the fit is loose. Proper placement involves passing both arms of the wedge to the other side. Given the Class 2 defect’s location in the middle area with equal tooth structure on both sides, a buccal-to-palatal wedge placement was used, following the classical approach. Figure 7
After placing and securing the band and wedge, photos were taken to ensure 100% seal.
Once the band is securely in place, the Quad ring is selected and positioned with its driver tip on the buccal side, following the placement of the wedge from the palatal. Figure 8
After completing the bonding procedure, a thin (approximately 0.5 mm) coat of Shofu Injectable XSL — a high-strength, self-levelling, second-generation injectable material — was applied to seal the dentine. This initial layer is essential for protecting the hybrid layer against polymerisation shrinkage stress. Thanks to its self-levelling nature, it adapts well to irregular surfaces, providing a smooth, bubble-free seal and helping to reduce post-operative sensitivity.
The restoration was then built up using an incremental anatomical layering technique with Shofu Beautifil LS II in shade A2. Finally, brown tint was added to mimic natural fissure staining and enhance the lifelike appearance of the restoration. After curing from all sides, the band and wedge are removed. Due to the rigidity of the band no excess flange and over contoured seen due to placing adjacent band. Figure 9
|
|
|
Figure 8. After Completion of restoring tooth#16 using incremental cusp by cusp buildup using Shofu Bioactive composite. Placement of FXH 175 firm band secured with the Quad orange wedge, checking the proximal seal.
| Figure 9. The Quad ring was placed with its driver tip from the buccal side.
|
The contours and embrasures were well established and finished using a Shofu Super Snap purple disk. The oxygen inhibition layer was removed using sodium bicarbonate powder with an air polisher unit.
A rubber dam was removed, and high points were checked using 40-micron paper, followed by 8-micron foil in static occlusion. For dynamic occlusion, 200-micron paper was used, and adjustments were made to the cuspal slopes and non-functional cusps. Finishing and Polishing Protocols:
- Finishing and margination of the occlusal surface were performed with a DuraGreen Stone.
- Polishing was done with SHOFU OneGloss MidiPoints.
- Super polishing was achieved with SuperBuff impregnated discs to provide a high gloss and an extra enamel-like luster.
|
|
|
| Figure 10. After restoring Class II defect | Figure 11. A different angle highlights the ideal height of the marginal ridge, with no excess composite and a natural-looking morphology.
|