Creating a correct contact area, both in terms of strength, extension, and location, is perhaps one of the fundamental needs, if not the most important one, in direct restorative dentistry. In 90% of cases, this area is created through the use of matrices that act as a “shell” to shape the form of the interproximal walls. This is essential to ensure proper function and long-term prognosis, avoiding issues such as early secondary caries, marginal leakage, and periodontal tissue inflammation (food impaction)..
We should remember that the fundamental requirements for achieving an optimal contact point are related to:
1. Perfect cervical seal
2. Correct emergence profile (divergent); Strong contact area in the correct position (to avoid black triangles)
3. Linear wall profile without deformation
These aspects can certainly be clinically evaluated at the time of wedge, matrix, and ring selection, but they are definitively confirmed by a well-centered bitewing radiograph taken at the final check.
To address these challenges in Class II direct restorations, Garrison® Dental Solutions introduced the Quad Matrix System™, an innovative solution designed to guarantee the above-mentioned characteristics while also saving clinical time. The real innovation lies not so much in the matrices, which can be selected from various categories within the brand based on their height and curvature radius, but rather in the wedge and, consequently, the ring. The wedge is bifurcated, snaketongue–shaped, slim yet robust, ensuring effective separation force. This design makes it ideal for all types of cavities. The advantages observed include:
- Excellent cervical seal in standard cavities
- Excellent cervical seal even in “non-standard” cavities, such as those with concave cervical steps when viewed occlusally
(bi-rooted premolars or certain molars on the mesial surface) - Reduced encroachment on the papilla due to the slimmer shape, allowing greater apical displacement
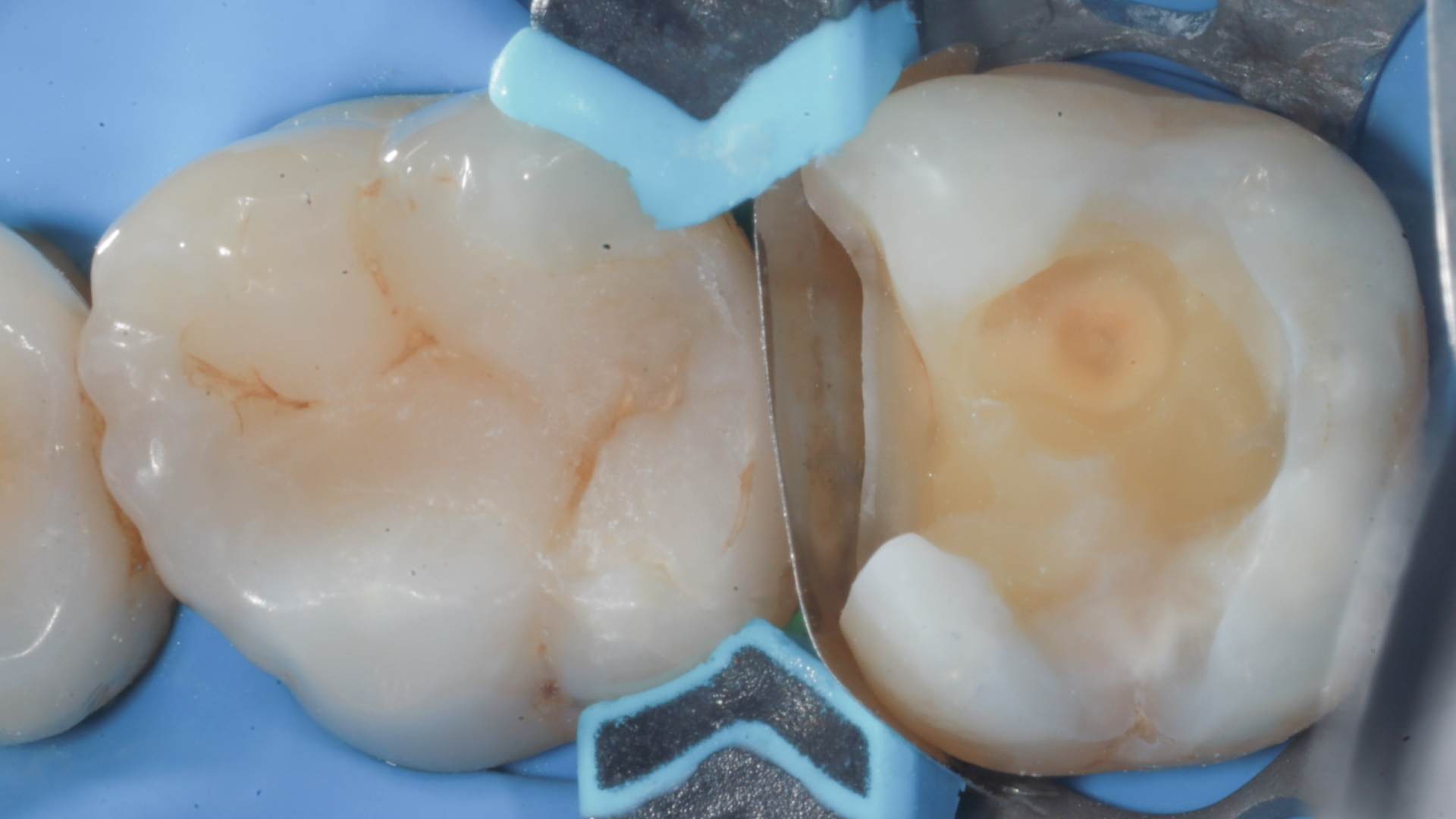
Once the wedge is placed (either buccally or palatally/lingually depending on clinical needs), it must be calculated to ensure a proper cervical seal, avoid matrix deformation, and allow the “bifurcation” of the wedge to emerge on the opposite side of insertion. At this point, the procedure is completed with the new asymmetric ring, which on one side features the classic wedge space, and on the other side a piston-like element capable of splitting the wedge, displacing the papilla, and ensuring an excellent cervical seal.
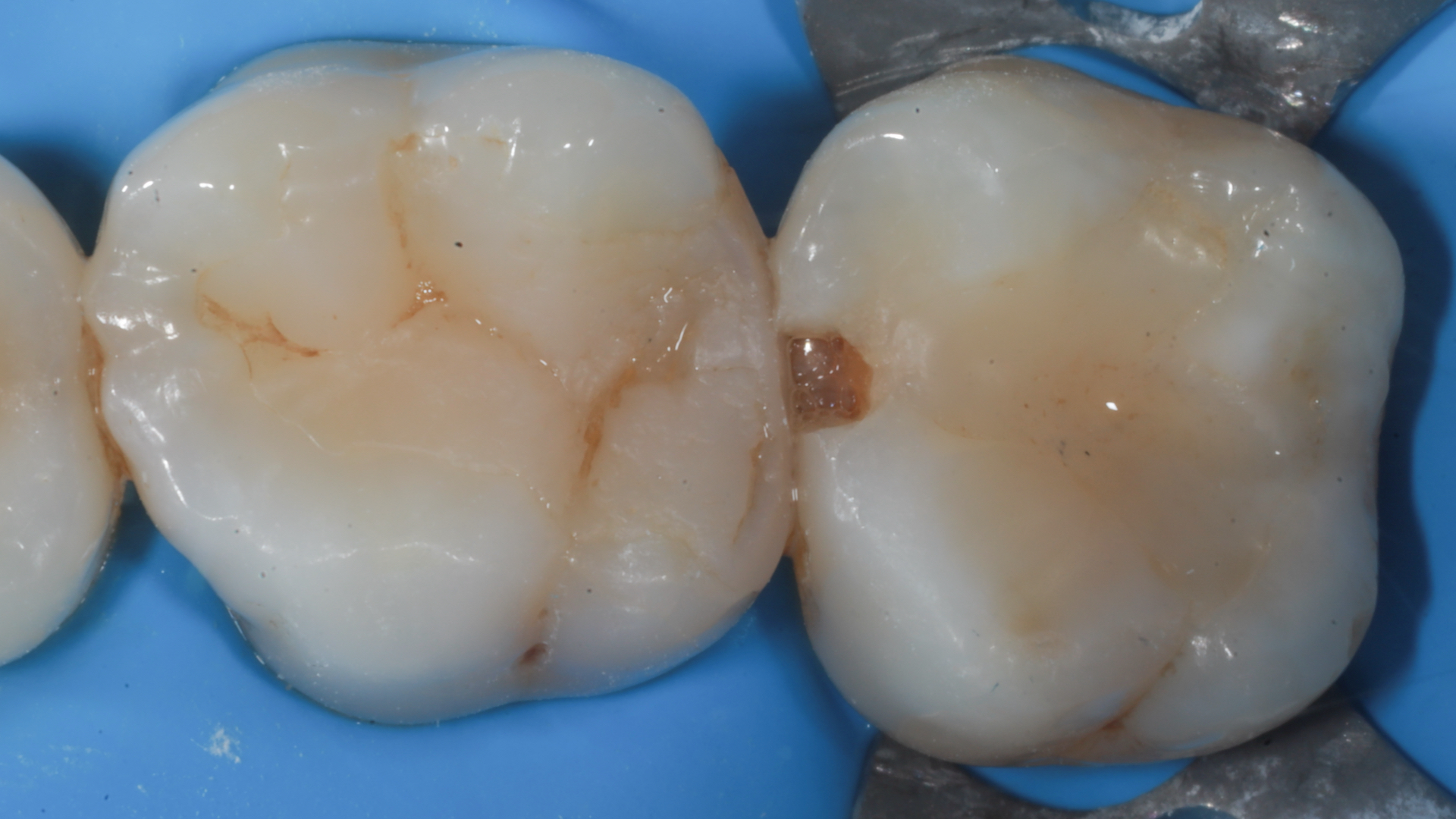
This clinical case illustrates the fundamental steps and the functional and esthetic rehabilitation achieved using this instrumentation: a mesial cavity on a maxillary second molar (an area where the bulk of the rubber dam clamp often prevents the use of other rings)