Restoring a Class 2 defect may seem simple—just place a slice of composite into the cavity and cure it—but this approach neglects crucial factors like contacts, contours, and gingival health. Any mistake in technique can compromise the entire quadrant, damaging both hard and soft tissues. Restoring Class 2 defects is one of the most complex challenges in restorative dentistry, and dealing with adjacent defects tests both your skills and knowledge. This case presentation demonstrates how to effectively restore improperly treated adjacent Class 2 defects using the right techniques, combined with the expertise required and the advanced Quad Matrix System from Garrison.
Introduction
Case History
A 62-year-old male presented to our dental office with complaints of gum pain in the maxillary right quadrant and an inability to chew effectively.
Clinical examination reveals composite restoration was done in between 1st molar and 2nd premolar. It looks like restoration just placed without any sectional matrix system joining both adjacent class 2 defect. The palatal view shows composite has placed directly on the gums which leading to gingival inflammation giving pain to the patient. Overall teeth shows signs of erosion with loss of good amount of enamel suggestive because of acid reflux.
Iopa reveals adjacent class 2 defect on tooth #15 & #16 with no close proximity to the nerve. The single composite restoration has placed in between these 2 defects.
Full Size Image

Full Size Image

Full Size Image

Isolation & Preparation of New Cavity designs for better adhesive techniques
- Rubber Dam Isolation: Use a wingless clamp with heavy rubber dam to achieve optimal bonding and increase the longevity of the restoration. Proper isolation is crucial for a successful adhesive process.
- Caries Removal: Utilize caries dye for the thorough removal of carious tissue in teeth #15, #16, Old composite is removed and infected caries is removed using slow speed round carbide bur. It is essential to establish a peripheral seal zone free from infected and affected dentine to ensure the best bonding strength.
- Enamel Preparation: Remove all unsupported enamel using a Super Fine Diamond Bur (yellow band). For new cavity designs, employ Cala Lilly burs, which are specifically engineered for adhesive composite restorations and designed to resist tooth fracturing.
- New Cavity design Technique: Following Dr. Richard Simonson’s concept, aim to avoid connecting the occlusal to the interproximal areas during first-time interproximal caries restoration (see pic 03). Finish the proximal walls with Shofu Super-Snap disks: start with the violet disk, followed by green and pink disks. This approach ensures optimal bonding to the enamel and helps prevent potential microleakage. Due to acid erosion the dentine turns into sclerotic leading to very poor bonding strength so decided to do a proper Air particle abrasion iusing 25-micron aluminum oxide powder for more than 10 secs. This process cleans the cavity preparation and enhances bonding strength, particularly by increasing some microporosity in the sclerotic dentine.
Full Size Image

Selecting the appropriate sectional matrix system is crucial in such adjacent large defect cases so we choose Garrison Quad system. It is essential to ensure that the marginal ridge is correctly dimensioned and aligns with the occlusal anatomy. This alignment is vital for creating well-defined adjacent triangular fossae and a properly shaped occlusal embrasure. Therefore, the height of the marginal ridge largely depends on the choice of band height. Here we choose Firm band FXH 200
The firmness of the band material facilitates easy placement and secure fitting, they bands maintain their shape and do not distort during the composite injection molding procedure, ensuring accurate and reliable restoration outcomes.
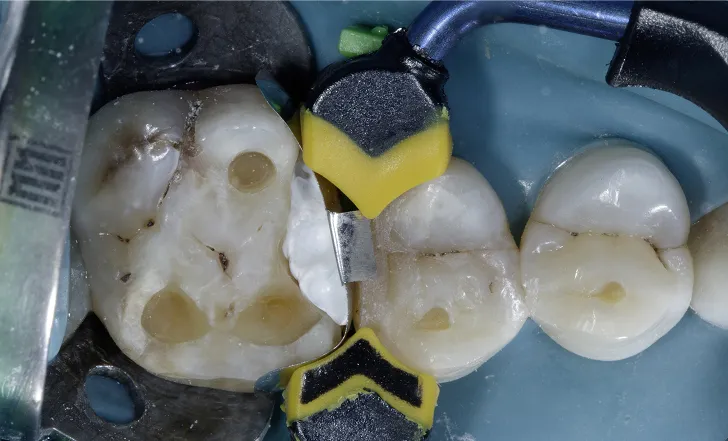
The first band (FXH 200) was placed in the distal defect of tooth #15 and secured using a Large Quad Wedge (Figure 05).
Next, an identical band was inserted into the mesial defect of tooth #16 by slightly repositioning the wedge, allowing the band to pass beneath it. The wedge was then reinserted to its full length, holding the bands in place with gentle finger pressure, ensuring both bands were securely positioned beneath the wedge. (Figure 05)
Full Size Image

Restoring #15
Since the adjacent defects are larger with larger interdental space, we decided to do the defect one by one. Due to small defect on tooth #15 compared to #16 we decided to do 1st #15 using injection molding technique without placing the matrix ring.
After applying the bonding agent, we used a thin layer of Shofu Injectable Xsl—a high-strength, self-levelling, 2nd generation injectable material—to seal the dentine. This initial layer, approximately 0.5 mm thick, is crucial for protecting the hybrid layer from shrinkage stress. The self-levelling properties of this material allow it to effectively adapt to uneven surfaces, ensuring a smooth application without air bubbles and minimizing post-operative sensitivity.
The 2nd increment we placed small quantity of Injectable Xsl A3O followed by packable composite Shofu Beautifil LS II A3.5 in injection molding technique manner. The excess composite is removed and marginal ridge is contoured properly.
After curing from all sides, the band and wedge are removed. Due to the rigidity of the band no excess flange and over contoured seen due to placing adjacent band. (Figure 07)
Full Size Image

Full Size Image

Restoring #16
Due to the larger defect on the palatal side compared to the buccal, we inserted the Quad large wedge from the palatal. The unique design of the wedge, with its broader area, ensures that the band is securely positioned at the wider defect, eliminating any gaps at the gingival seat area. (Figure 08)
Once the band is securely in place, the Quad ring is selected and positioned with its driver tip on the buccal side, following the placement of the wedge from the palatal. Teflon tape is then placed inside the defect to shape the band to the adjacent tooth, ensuring ideal contour and contact. (Figure 09)
Full Size Image

Full Size Image
The bonding process and a thin layer of Shofu Injectable Xsl were applied in the same manner as for tooth #15. Due to the larger defect, we decided to convert the Class 2 into a Class 1 by first creating the wall. To achieve this, we used the snow plow technique with a stress-reducing layering approach. This involved building the walls separately on the palatal and buccal sides using Shofu Injectable XSL A3O and Packable Shofu Beautifil LS II A3.5. (Figure 10)
The remaining defect is restored using the same snow plow technique. Additionally, the occlusal erosion facets are also restored.
The contours and embrasures were well established and finished using a Shofu Super Snap purple disk. The oxygen inhibition layer was removed using sodium bicarbonate powder with an air polisher unit. (Figure 11)
Full Size Image

Full Size Image

Full Size Image

A large soft tissue defect is visible due to the faulty restoration. With the newly restored teeth, this will support healing and promote soft tissue growth. (Figure 13)
The patient was recalled after two weeks for a soft tissue assessment, where it was noted that the interdental papilla had grown back naturally. (Figure 12)
This wasn’t a miracle, but rather the result of using the proper technique with the Quad matrix. The patient was advised to use a water flosser to maintain regular oral hygiene and was also encouraged to consult a physician about his gastric reflux to prevent further enamel damage.
Full Size Image

Full Size Image

Full Size Image

Full Size Image

Full Size Image

Full Size Image

Full Size Image