FREE SHIPPING on orders over $475
FREE SHIPPING on orders over $475 | No Code Needed
IntroductionQuadrant rehabilitation involving multiple teeth with varying restorative requirements remains one of the most demanding procedures in restorative dentistry. Differences in cavity design, proximal defect configuration, aesthetic demands, and restorative modalities often necessitate the use of different matrix systems within the same treatment session. Appropriate matrix selection plays a crucial role in achieving optimal proximal contact, contour, emergence profile, and restorative predictability. This article presents a comprehensive quadrant rehabilitation in which three different matrix systems were employed for the management of multiple direct and indirect restorations. The clinical workflow, rationale for matrix selection, and restorative outcomes are presented, together with a five-year clinical and radiographic follow-up demonstrating the long-term stability of the treatment. Case HistoryA 30-year-old female patient presented to the dental clinic with a chief complaint of pain associated with tooth #46. The pain was intermittent in nature and occasionally sharp during mastication or application of pressure. Clinical examination revealed a multi-surface defect involving tooth #46, which exhibited tenderness to percussion. An adjacent Class II carious lesion was observed on the distal aspect of tooth #45 and mesial aspect already restored with the composite. Tooth #47 demonstrated a failing composite restoration with loss of lingual tooth structure, likely resulting from cusp fracture or structural weakening. In addition, inadequate proximal contacts and improper contours were noted, contributing to food impaction and plaque accumulation. These factors, combined with the patient’s high caries risk and suboptimal oral hygiene, appeared to have contributed to the development of multiple restorative defects within the quadrant. (Figure 01) Radiographic evaluation using an intraoral periapical radiograph (IOPA) revealed pulpal involvement of tooth #46, a distal proximal lesion associated with tooth #45, and recurrent caries beneath the existing restoration on tooth #47, particularly involving the mesial proximal box. (Figure 01) |

|
| Figure 1: Intraoral mirror-reflected view of the mandibular right posterior quadrant demonstrating multiple restorative defects involving teeth #45 and #47, along with endodontic involvement of tooth #46. |
Treatment PlanningA phased treatment approach was planned and completed over only three clinical appointments. During the first appointment, endodontic treatment of tooth #46 was performed to eliminate pain and infection. Following resolution of symptoms, the second appointment was scheduled for the restoration of teeth #45, #46, and #47. During the same visit, tooth preparation and impression making for the definitive full-coverage restoration of tooth #46 were completed. The third appointment involved placement of the definitive crown, followed by occlusal adjustment and verification of functional harmony. Considering the patient’s high caries risk, history of recurrent restorations, and inadequate oral hygiene maintenance, a minimally invasive treatment philosophy was adopted. Whenever feasible, bonded adhesive restorations were preferred to preserve maximum tooth structure while providing predictable functional and aesthetic outcomes. Clinical ProcedureAppointment 01 – Root Canal of tooth #46Considering the patient’s chief complaint, clinical findings, and radiographic evidence of pulpal involvement, tooth #46 was referred for endodontic treatment. Root canal therapy was completed by an endodontic specialist to eliminate pain and infection and to establish a stable foundation for the subsequent restorative procedures. The patient was recalled after one week for reassessment. As the tooth remained asymptomatic and free from tenderness to percussion, definitive restorative treatment was initiated. Appointment 02 – Direct Restoration phase for tooth #45,46,47Following completion of endodontic treatment and resolution of symptoms, the patient returned after one week for the restorative phase involving teeth #45, #46, and #47. In quadrant dentistry, it is often advantageous to initiate treatment from the most posterior tooth. This approach facilitates better operator access and visibility, while minimizing patient fatigue associated with prolonged mouth opening during the later stages of the procedure. Tissue contouring was performed using electrocautery to recreate a physiologic gingival architecture and to clearly expose the proximal defects. Tooth #45Existing composite material was selectively removed from the occlusal surface, followed by complete caries excavation of the distal lesion to create a conventional Class II cavity preparation. The mesial composite restoration was clinically intact and free from discoloration, marginal breakdown, or recurrent caries; therefore, it was preserved. |
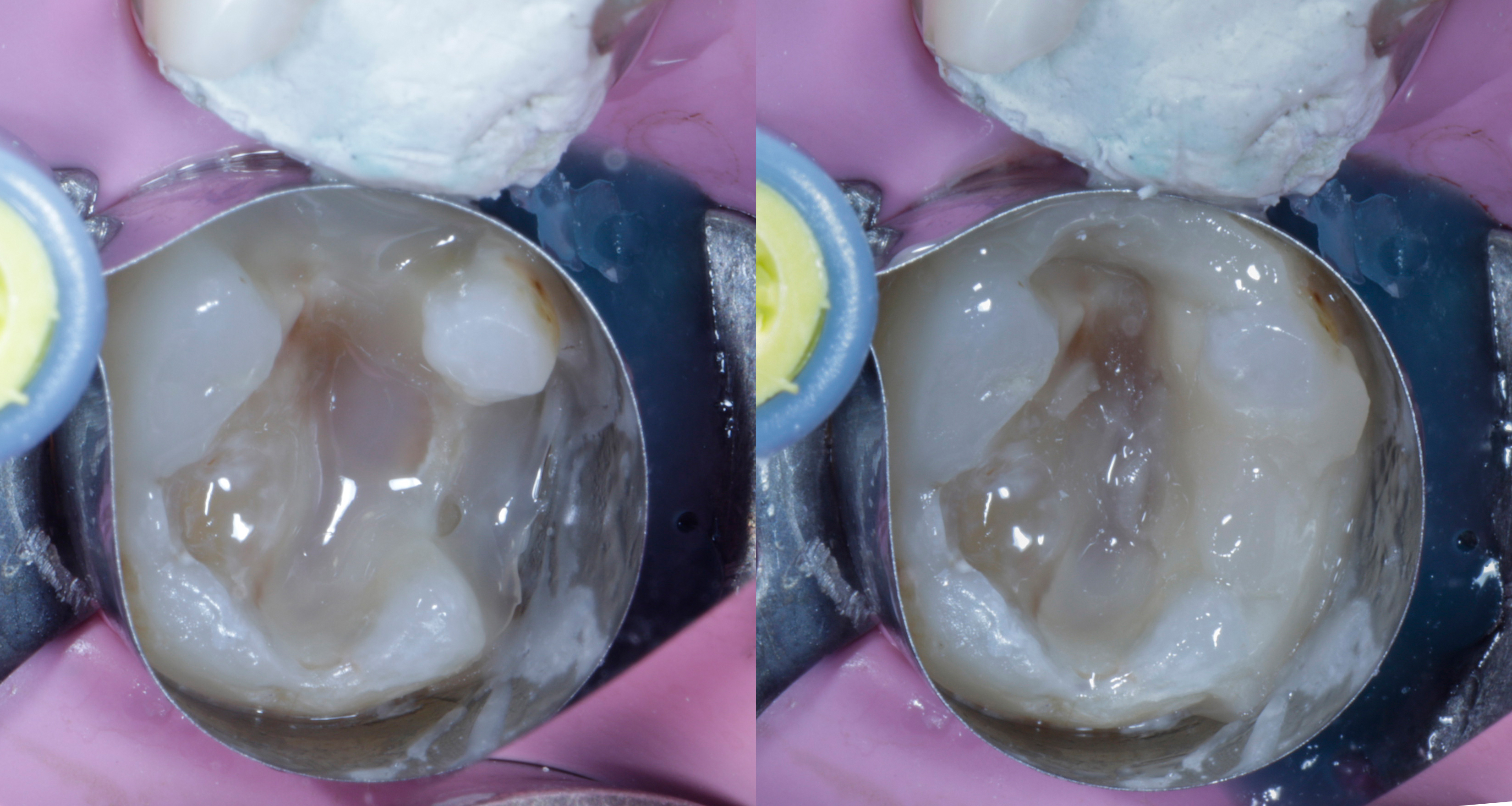
Tooth #47The existing restoration and underlying carious dentin were removed using a combination of rotary instrumentation and caries-detecting dye. Areas of weakened tooth structure, particularly along the lingual aspect, were eliminated. Unsupported enamel margins were refined, and the cavity preparation was finished using abrasive discs to obtain smooth and well-defined restorative margins. A heavy-gauge rubber dam was placed using a wingless clamp to achieve optimal isolation and moisture control. Effective isolation is critical for the success and longevity of adhesive restorations, particularly during extensive quadrant rehabilitation procedures. In addition to providing a contamination-free operating field, rubber dam isolation enhances visibility, improves operator efficiency, and increases patient comfort during prolonged treatment sessions. Both preparations were air-abraded using 50-µm aluminum oxide particles for approximately 5–7 seconds, followed by thorough rinsing and drying. Selective enamel etching was then performed, after which the cavities were rinsed for 20 seconds and carefully cleaned prior to adhesive application (Figure 2). |

|
| Figure 2: Rubber dam isolation and cavity preparation of teeth #45 and #47 following caries removal, air abrasion, and selective enamel etching. The teeth are prepared and ready for adhesive restoration and composite layering. |
| A clinical challenge was encountered in tooth #47 due to the presence of both a mesial proximal defect and a lingual structural deficiency. Although a conventional Tofflemire matrix could have been used, its flat matrix band often limits the reproduction of natural proximal contours. Therefore, a Garrison ReelMatrix system was selected. The pre-contoured, thin matrix band allowed rapid adaptation and facilitated the creation of a more anatomical proximal wall (Figure 3). |

|
| Figure 3: ReelMatrix adapted around tooth #47 to manage the combined proximal and lingual defect. Complete circumferential (360°) sealing was achieved using the matrix system in conjunction with liquid dam, providing optimal isolation for the adhesive restorative procedure. |
As the lingual margin extended slightly subgingivally, a portion of the rubber dam was carefully trimmed to improve access and visualization. The ReelMatrix band was adapted around the tooth, and any remaining openings were sealed using a liquid dam material. This technique provided complete circumferential isolation and ensured a secure operative field prior to adhesive application and composite layering. Following the adhesive protocol, a thin adaptation layer of injectable composite (Beautifil Injectable XSL, Shade A2O, Shofu) was applied to the cavity floor and dentinal surfaces. Owing to its excellent flow characteristics and slow-leveling behavior, the material readily adapted to internal irregularities, line angles, and cavity walls, minimizing the risk of voids and enhancing interfacial adaptation. The composite was applied in a thickness of approximately 0.5 mm and light-cured according to the manufacturer’s recommendations. This thin adaptation layer promotes intimate contact with the dentin substrate, reduces the volume of material polymerized in a single increment, and helps mitigate polymerization shrinkage stresses. Furthermore, it acts as a stress-absorbing layer, protecting the adhesive interface and hybrid layer during subsequent restorative build-up. Following dentin sealing, the proximal wall and lingual defect were reconstructed to convert the complex cavity configuration into a more manageable Class I preparation. Establishing the proximal contour and marginal ridge at this stage simplified the subsequent occlusal layering procedure and allowed for more controlled anatomical reconstruction. For this purpose, a highly filled packable composite resin (Beautifil LS II, Shofu) was selected. With a filler loading of approximately 87–88 wt% and reported polymerization shrinkage of only 0.85%, the material offers excellent mechanical properties, wear resistance, and dimensional stability, making it suitable for stress-bearing posterior restorations (Figure 4). |
|
| Figure 4: Clinical view following immediate dentin sealing (IDS) and defect reconstruction with injectable and packable composite resins (Shofu). Restoration of the proximal and lingual walls transformed the extensive multi-surface defect into a Class I configuration, enabling predictable cusp-by-cusp anatomical layering. |
Based on the extent and configuration of the defect, polyethylene reinforcement fibers (Ribbond, Seattle, USA) pre-wetted with unfilled resin were incorporated within the restoration and light-cured (Figure 7). Fiber reinforcement was considered advantageous due to the large cavity size and unfavorable cavity configuration factor (C-factor). The incorporation of Ribbond fibers has been shown to enhance fracture resistance, limit crack propagation within the composite restoration, and improve stress distribution across both the restorative material and the remaining tooth structure. These benefits are particularly relevant in structurally compromised teeth and extensive posterior restorations. Following fiber placement, the restoration was completed using an incremental cusp-by-cusp layering technique with Beautifil LS II. This approach facilitated precise anatomical reconstruction while minimizing polymerization stress and ensuring adequate depth of cure. |

|
| Figure 6: Cusp-by-cusp morphological layering technique performed following conversion of the defect into a Class I configuration, allowing precise anatomical reconstruction of the posterior tooth structure. |

|
| Figure 7: FX175 sectional matrix band secured with a Garrison 3D Fusion ring, demonstrating complete cervical sealing and optimal proximal adaptation prior to adhesive restoration of tooth #45. |
Upon completion of tooth #47, attention was directed to tooth #45. An FX175 sectional matrix band was adapted and stabilized using a Garrison wedge. Once the proximal box was effectively sealed, a Garrison 3D Fusion ring was placed to achieve optimal matrix adaptation and tooth separation. After verification of a complete cervical seal, the same adhesive and restorative protocol described for tooth #47 was followed. The proximal wall was first reconstructed to convert the Class II cavity into a Class I configuration, followed by incremental anatomical layering of the composite resin. Following polymerization, only minimal contour refinement and finishing were required due to the accurate reproduction of the proximal and occlusal anatomy. |
Tooth #46 – Deep Margin Elevation and Core Build-UpFollowing complete caries excavation, the cavity was refined and air-abraded using 50-µm aluminum oxide particles. Selective enamel etching was subsequently performed according to the previously described adhesive protocol (Figure 9). |

|
| Figure 8: Final clinical outcome of tooth #45 following restoration, illustrating harmonious integration of form and function with proper proximal contour, contact integrity, and anatomical occlusal morphology. |
Tooth #46 – Deep Margin Elevation and Core Build-UpFollowing complete caries excavation, the cavity was refined and air-abraded using 50-µm aluminum oxide particles. Selective enamel etching was subsequently performed according to the previously described adhesive protocol (Figure 9). The most challenging aspect of this restoration was the deep distal margin, which extended subgingivally. Initial soft tissue management was performed using electrocautery, allowing improved visualization, access, and isolation of the cervical margin. Following adequate tissue control, a Deep Margin Elevation (DME) procedure was planned. Deep Margin Elevation is a conservative restorative approach in which a deep cervical margin is relocated coronally using adhesive composite resin. This technique facilitates subsequent isolation, impression making, and adhesive cementation procedures by converting a difficult subgingival margin into an equigingival or supragingival one. To accomplish this, a dedicated Garrison Deep Margin Elevation matrix system was utilized. The pre-contoured rigid matrix provided excellent adaptation to the deep cervical area, allowing predictable sealing of the subgingival margin and controlled placement of the restorative material. The matrix design enabled stable positioning and accurate emergence profile development while minimizing the need for more invasive surgical procedures such as crown lengthening. Following matrix placement, careful verification of the cervical seal was performed, as marginal adaptation is critical to the long-term success of the DME procedure. After adhesive application, the bonding agent was actively rubbed into the dentin surface for more than 20 seconds to enhance substrate interaction and maximize bond strength in this challenging deep cervical region. |

|
| Figure 10: Garrison Deep Margin Elevation (DME) matrix band positioned on tooth #46, providing stable adaptation to the deep cervical margin and enabling controlled composite placement for margin relocation. |
As previously described, a thin adaptation layer of injectable composite was first applied to ensure intimate adaptation and complete sealing of the cavity floor. Incremental placement of a highly filled packable composite (Beautifil LS II, Shofu) was then used to elevate the distal margin and establish a stable cervical platform. Once the deep margin was successfully relocated, the remaining cavity volume was restored using a dual-cure core build-up composite. The material was allowed to self-cure for approximately three minutes before light activation, thereby reducing polymerization stress development and ensuring complete curing throughout the restoration. Given the extensive loss of tooth structure, history of high caries activity, some demineralisation cervical enamel and compromised oral hygiene status, a full-coverage indirect restoration was planned for tooth #46. Tooth preparation was performed under rubber dam isolation, allowing precise margin placement in a supragingival position and facilitating subsequent adhesive procedures. Upon completion of the restorative phase, the rubber dam was removed and occlusion was carefully evaluated. Any premature contacts were adjusted, and all direct restorations were finished and polished. A final impression was then obtained for fabrication of the definitive crown, and a provisional restoration was delivered to protect the preparation and maintain positional stability until the definitive restoration could be placed. |

|
| Figure 12: Completion of the adhesive core build-up. Following Deep Margin Elevation and reconstruction of the cavity walls, the residual defect was restored with a dual-cure core composite to establish adequate structural support for the definitive indirect restoration. |
Appointment 03 – Adhesive Cementation of the Definitive Restoration for Tooth #46The patient was recalled one week later for placement of the definitive full-coverage restoration. A lithium disilicate glass-ceramic crown was selected because of its favorable mechanical properties, excellent esthetics, and optical characteristics that closely resemble natural enamel. Rubber dam isolation was achieved without difficulty due to the previously completed deep margin elevation procedure and the supragingival preparation design. This facilitated predictable moisture control during the adhesive cementation procedure. The tooth preparation was air-abraded using 50-µm aluminum oxide particles to remove residual temporary cement, biofilm, and surface contaminants. Proper preparation of the bonding substrate is essential, as the long-term success of adhesive cementation is highly dependent on the cleanliness and quality of the prepared tooth surface (Image 14). |

|
| Figure 14: Air-abraded tooth preparation ready for bonding. Note the clean substrate and predominantly enamel margins, with DME composite present at the distal margin. |
The intaglio surface of the lithium disilicate restoration was conditioned according to the manufacturer’s recommendations. The surface was air-abraded, ultrasonically cleaned, etched with hydrofluoric acid, thoroughly rinsed, and subjected to a second ultrasonic cleaning cycle. Following drying, a silane coupling agent was applied for 60 seconds to promote durable chemical bonding between the ceramic and resin-based luting material. The tooth surface was then treated with the adhesive system according to the manufacturer’s protocol. A bonding agent was applied and light-cured prior to crown placement. For cementation, a highly filled injectable composite resin (Beautifil Injectable X, Shofu) was utilized as the luting medium. The material offers favorable handling characteristics, excellent polishability at supragingival margins, and controlled viscosity that facilitates complete seating while minimizing excessive material extrusion. In addition, its light-curing capability provides extended working time, allowing meticulous removal of excess material from the margins and proximal contacts before final polymerization. Unlike direct intracoronal restorations, the luting composite is present as a thin film between the tooth and restoration, resulting in a more favorable C-factor and reduced polymerization shrinkage stress during curing. The restoration was filled with an adequate quantity of composite resin and seated onto the prepared tooth. Initial seating pressure was applied, followed by removal of gross excess material. Additional seating pressure was then maintained to ensure complete adaptation of the restoration. Excess composite was removed from the margins using suitable hand instruments and microbrushes. Particular attention was given to the proximal contact areas. Dental floss was carefully passed through each contact while maintaining constant seating pressure on the restoration to prevent displacement. This maneuver was repeated several times to ensure complete removal of excess resin from the interproximal regions. A brief tack cure of approximately three seconds was performed to facilitate further cleanup of residual material. Glycerin gel was subsequently applied to all restoration margins to eliminate the oxygen-inhibited layer and promote complete polymerization. Final light curing was carried out from all accessible aspects for 20 seconds per surface using a high-intensity curing unit. Following removal of the rubber dam, occlusion was carefully evaluated in both static and dynamic movements using articulating papers of varying thicknesses. Any premature contacts were adjusted using fine-grit diamond finishing instruments designed for ceramic restorations. Final polishing was completed using dedicated ceramic polishing systems to restore a smooth, high-gloss surface and minimize wear of the opposing dentition. A postoperative periapical radiograph was obtained to verify complete seating of the restoration and confirm the absence of residual excess luting material within the proximal regions. |

|
| Figure 15: Final clinical outcome following adhesive cementation and occlusal adjustment of the lithium disilicate crown. Postoperative radiographs confirm complete seating of the restoration and absence of residual excess composite cement. |

|
| Figure 16: Color-coded radiographic illustration depicting the restorative complex: red indicates the Deep Margin Elevation (DME), yellow represents the dual-cure core build-up composite, and blue denotes the definitive lithium disilicate ceramic crown. |

|
| Figure 18: Comparative preoperative and postoperative clinical views illustrating the transformation of the quadrant and the re-establishment of functional and anatomical tooth morphology. |
Five-Year Clinical Follow-UpThe patient returned for clinical and radiographic evaluation approximately five years after completion of treatment. Clinical examination revealed that all restorations remained functional and asymptomatic. The bonded lithium disilicate crown on tooth #46 demonstrated satisfactory marginal integrity with no evidence of debonding, fracture, or secondary caries. The direct composite restorations on teeth #45 and #47 maintained acceptable anatomical form, proximal contacts, and occlusal function. Periodontal tissues surrounding the restored teeth appeared healthy, with no adverse effects associated with the Deep Margin Elevation procedure. Follow-up radiographs demonstrated stable periapical and restorative conditions with no evidence of recurrent caries or marginal breakdown. The patient reported complete satisfaction with both function and aesthetics. DiscussionSuccessful quadrant rehabilitation often requires management of multiple defect configurations within the same treatment session. As demonstrated in this case, no single matrix system can predictably address every restorative challenge. Matrix selection should therefore be guided by the morphology and location of the defect rather than a one-system-fits-all approach. The complex proximal-lingual defect in tooth #47 was managed using the Garrison ReelMatrix system, which provided circumferential adaptation and facilitated predictable reconstruction of the missing walls. In contrast, the Class II lesion in tooth #45 was restored using a sectional matrix system (FX175 band with Garrison 3D Fusion ring) to achieve optimal proximal contours and contact formation. For tooth #46, the presence of a deep subgingival margin necessitated the use of a dedicated Deep Margin Elevation (DME) matrix, allowing predictable margin relocation and simplifying subsequent adhesive procedures. A key restorative principle throughout treatment was the conversion of complex cavity designs into simpler Class I configurations before final occlusal reconstruction. Immediate dentin sealing, wall reconstruction, and incremental composite placement facilitated improved control of polymerization stress while enhancing anatomical predictability. In extensive defects, incorporation of polyethylene fiber reinforcement may further contribute to stress distribution and restoration reinforcement. The DME procedure played a critical role in the management of tooth #46. Relocating the deep cervical margin to a more accessible position simplified isolation, impression making, and adhesive cementation while preserving the surrounding periodontal tissues. Furthermore, the restorative strategy followed a biomimetic philosophy in which composite resin replaced lost dentin and a bonded lithium disilicate crown replaced enamel. The combination of adhesive procedures, fiber reinforcement, composite build-up, and bonded ceramic restoration created a cohesive restorative complex designed to preserve tooth structure while restoring function and biomechanics. The favorable five-year clinical and radiographic follow-up demonstrated stable restorations, maintained proximal contacts and contours, healthy surrounding tissues, and absence of recurrent caries or restorative complications. These findings support the long-term predictability of combining appropriate matrix selection with contemporary adhesive restorative protocols in the management of complex restorative cases. ConclusionThis case demonstrates how successful quadrant rehabilitation often requires the integration of multiple restorative strategies tailored to the specific defect configuration of each tooth. The use of three different Garrison matrix systems enabled predictable management of a conventional Class II restoration, a complex proximal-lingual defect, and a deep subgingival margin requiring Deep Margin Elevation (DME). By combining adhesive restorative principles, immediate dentin sealing, fiber reinforcement, DME, and a bonded lithium disilicate crown, a biomimetic restorative approach was achieved while preserving maximum tooth structure. Careful matrix selection, meticulous isolation, and appropriate adhesive protocols were key factors in restoring form, function, proximal anatomy, and long-term restorative predictability. This case highlights that successful quadrant rehabilitation is not dependent on a single matrix system, but rather on selecting the right matrix solution for each clinical challenge. The favorable five-year clinical and radiographic follow-up demonstrated stable restorations, maintained proximal contacts and contours, healthy surrounding tissues, and absence of recurrent caries or restorative complications. This case highlights that successful quadrant rehabilitation is not dependent on a single matrix system, but rather on selecting the appropriate matrix solution for each clinical challenge and combining it with sound adhesive restorative principles.
Reference1. Magne P. Immediate dentin sealing: A fundamental procedure for indirect bonded restorations. Journal of Esthetic and Restorative Dentistry. 2005;17(3):144-155. 2. Magne P, Douglas WH. Porcelain veneers: Dentin bonding optimization and biomimetic recovery of the crown. International Journal of Prosthodontics. 1999;12(2):111-121. 3. Dietschi D, Spreafico R. Current Clinical Concepts for Adhesive Cementation of Tooth-Colored Restorations. Practical Periodontics and Aesthetic Dentistry. 1998;10(1):47-54. 4. Bertoldi C, Monari E, Cortellini D, Generali L. Deep Margin Elevation: A systematic review and clinical considerations. Operative Dentistry. 2020;45(6):E336-E346. 5. Veneziani M. Adhesive restorations in the posterior area with subgingival cervical margins: New classification and differentiated treatment approach. European Journal of Esthetic Dentistry. 2010;5(1):50-76. 6. Rocca GT, Krejci I. Bonded indirect restorations for posterior teeth: From cavity preparation to provisionalization. Quintessence International. 2007;38(5):371-379. 7. Rocca GT, Rizcalla N, Krejci I, Dietschi D. Evidence supporting Deep Margin Elevation. Operative Dentistry. 2012;37(6):597-606. 8. Garoushi S, Vallittu PK, Lassila LVJ. Short fiber-reinforced composite restorations: A review of the literature. Journal of Investigative and Clinical Dentistry. 2018;9(4):e12330. 9. Belli S, Cobankara FK, Eraslan O, Eskitascioglu G, Karbhari V. The effect of fiber insertion on fracture resistance of endodontically treated molars restored with composite. Journal of Biomedical Materials Research Part B. 2006;78B(1):73-80. 10. Magne P, Belser UC. Bonded Porcelain Restorations in the Anterior Dentition: A Biomimetic Approach. Quintessence Publishing; 2002. 11. Magne P, So WS, Cascione D. Immediate dentin sealing supports higher bond strength and improved restoration longevity. Journal of Prosthetic Dentistry. 2007;97(1):1-6. 12. Guess PC, Selz CF, Voulgarakis A, Stampf S, Stappert CFJ. Prospective clinical study of lithium disilicate all-ceramic crowns. International Journal of Prosthodontics. 2013;26(5):435-442. 13. Sailer I, Makarov NA, Thoma DS, Zwahlen M, Pjetursson BE. All-ceramic or metal-ceramic tooth-supported fixed dental prostheses? A systematic review of survival and complication rates. Dental Materials. 2015;31(6):603-623. 14. Magne P. Biomimetic restorative dentistry: The bond of life. Quintessence Publishing; 2021. 15. Pascal Magne. Biomimetic Dentistry Mastership. Quintessence Publishing; selected chapters on IDS, stress distribution, and bonded indirect restorations. |


